
Our Workflow
Transmission of Measurement and
Clinical Forms to Us:
After becoming a member of our website, you can select the package you want to process and follow the steps on the website to upload the necessary photos, clinical analysis form, radiographs and videos.
After the records we receive, we start the planning of orthodontics and/or orthognathic surgery before mutual orthognathic surgery with an online meeting request. After the planning is completed, we produce the surgical splints to be used in the surgery after a joint meeting with you.
Necessary Registrations
Before You Start
Online
Examination Form
Photo
and Video
Records
Intraoral Scanning
and Bite
Scanning
Prepare the Patient for Tomography
Prepare Data
and Make a Planning
Appointment
The success of 3D digital planning is directly proportional to the sensitivity of the records to be collected. We recommend taking the records at least 2 weeks before the surgery. This way, we will have enough time to plan the orthognathic surgery, evaluate your patient together and prepare the surgical splints.
The records to be taken for successful planning and the issues to be considered during this process are explained in detail below. We recommend that you read this workflow before you start taking records.
We strongly recommend that you read this workflow before you start recording.
Video recording from the patient before orthognathic surgery is important for better planning of the surgical intervention. Here are some points where this video recording is important:
Facial Analysis: It can be used to dynamically evaluate the patient's facial expressions, jaw movements, smile aesthetics and general facial features.
Speech Analysis: It can be used to evaluate the patient's jaw and muscle movements that occur during speech and any problems that may occur during speech.
Understanding Patient Expectations: It allows us to better understand the patient's expectations after surgery. It also allows us to test whether the patient is sufficiently informed about the surgical procedure.
Recommended questions to ask the patient during the video recording:
- Why did you decide to have surgery?
- What do you want to change about your face and teeth?
- What do you know about complications that may occur during and after the surgery?
- What do you know about the postoperative period?
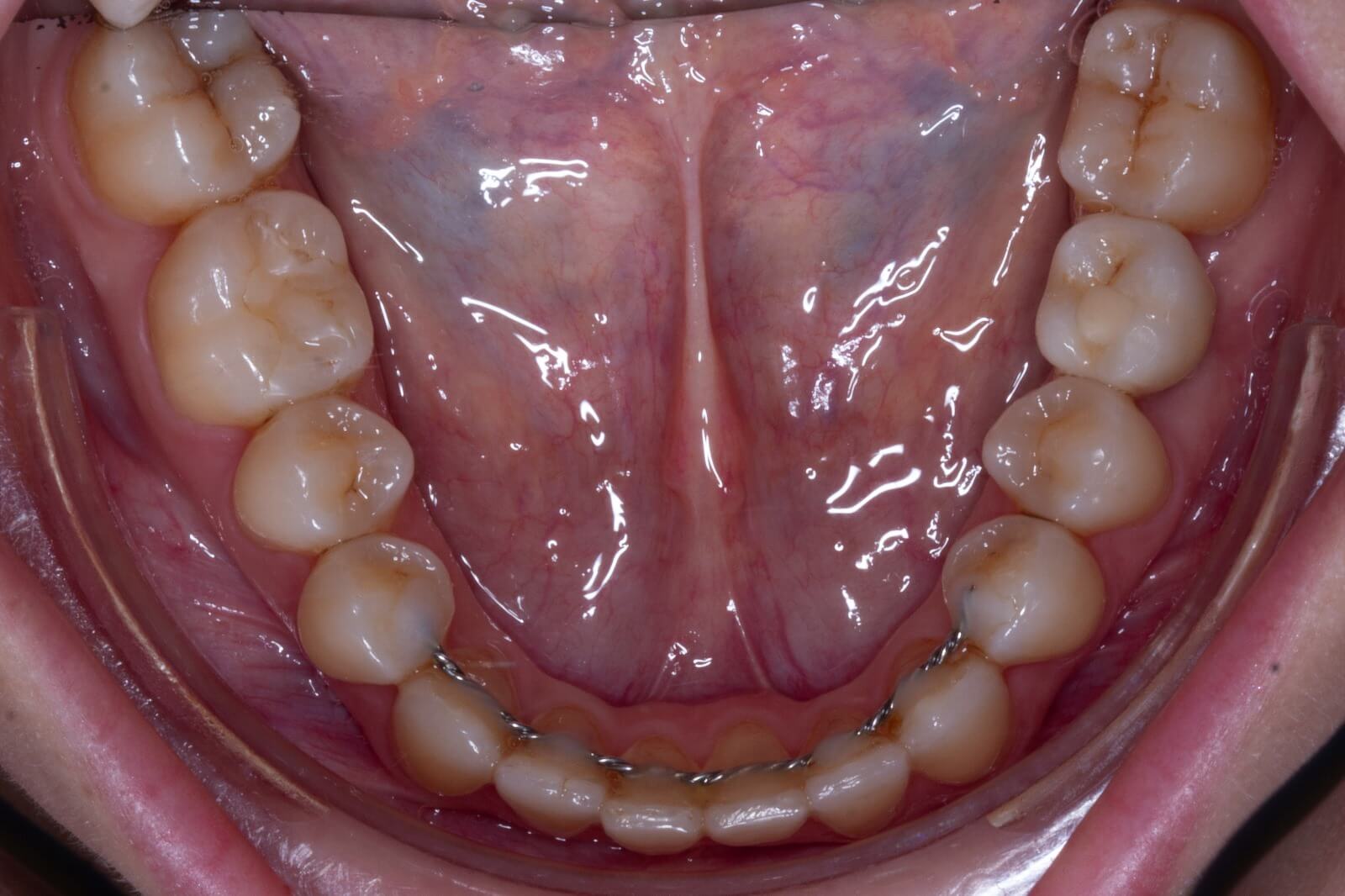
Before you start collecting the next set of records, we recommend that you take an impression with alginate and check one last time that the models have the proper occlusion. If there are minor discrepancies, these should be corrected with negative or positive coronoplasty to achieve a stable bite. When taking alginate impressions, the retentive areas between the bracket and the gingiva should be carefully covered with pink wax so that the alginate is not deformed during the impression making process. In addition, applying a special adhesive varnish to the impression spoon before placing the alginate will increase the reliability of the impression.
In order to produce surgical splints accurately, the intraoral scanning must be performed precisely. Before scanning, oral hygiene should be good, there should be no saliva on the surfaces to be scanned, and the elastic on the teeth should be removed. We do not recommend removing the surgical arches. Because the passivity of the arches may be impaired during the removal and insertion of the surgical arches. Any tooth movement that may occur after the records are taken will cause the surgical splints not to fit properly on the teeth. Before the intraoral scanning of clear aligner patients, we recommend that you discuss with the surgeon which method he/she wants to use to connect the jaws. Some surgeons prefer to attach brackets to the teeth, some prefer to attach wires with hooks or to be supported only by mini screws. In this case, a final intraoral scan should be performed according to the desired method.
The scanning device must be calibrated.
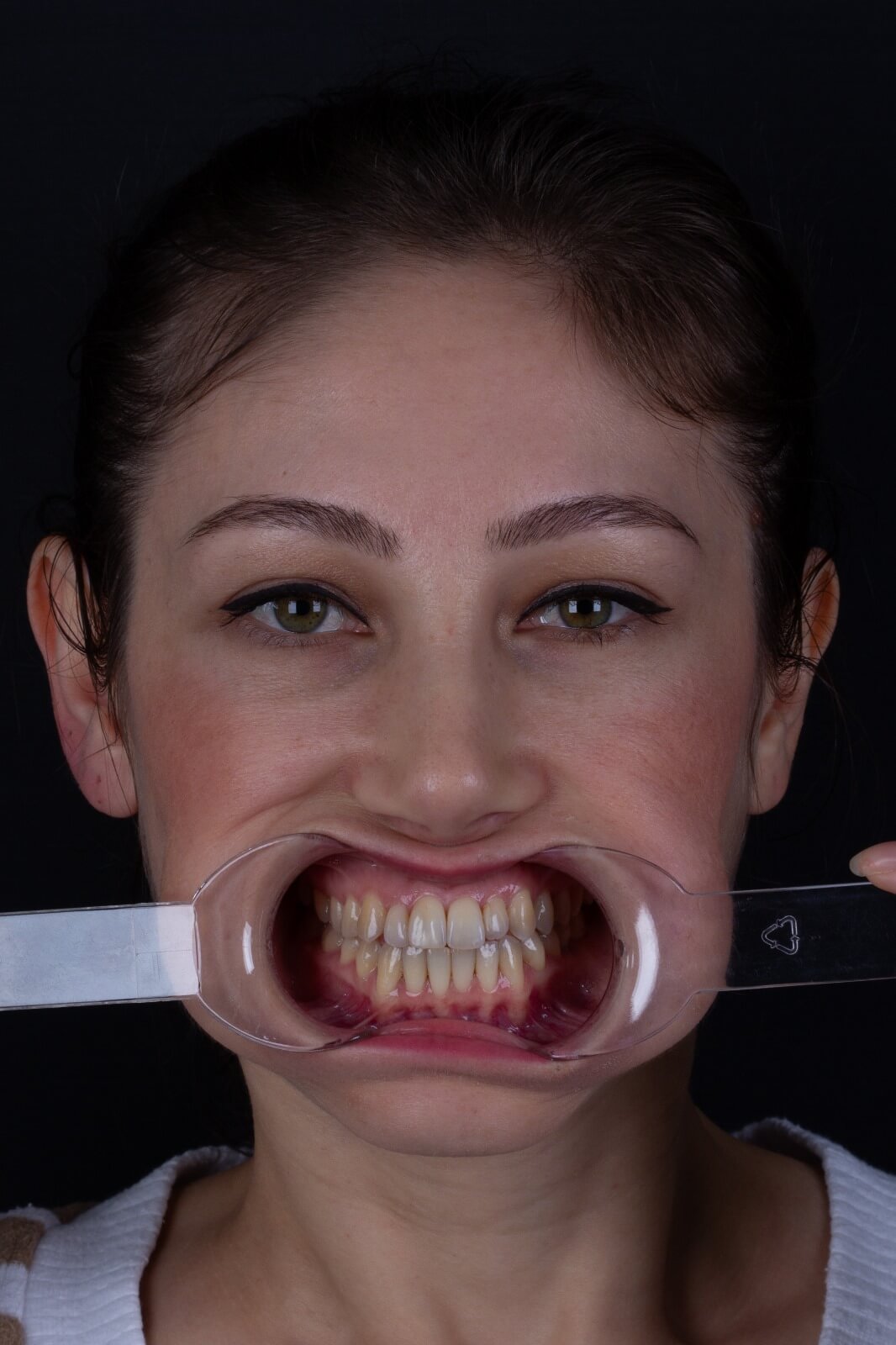
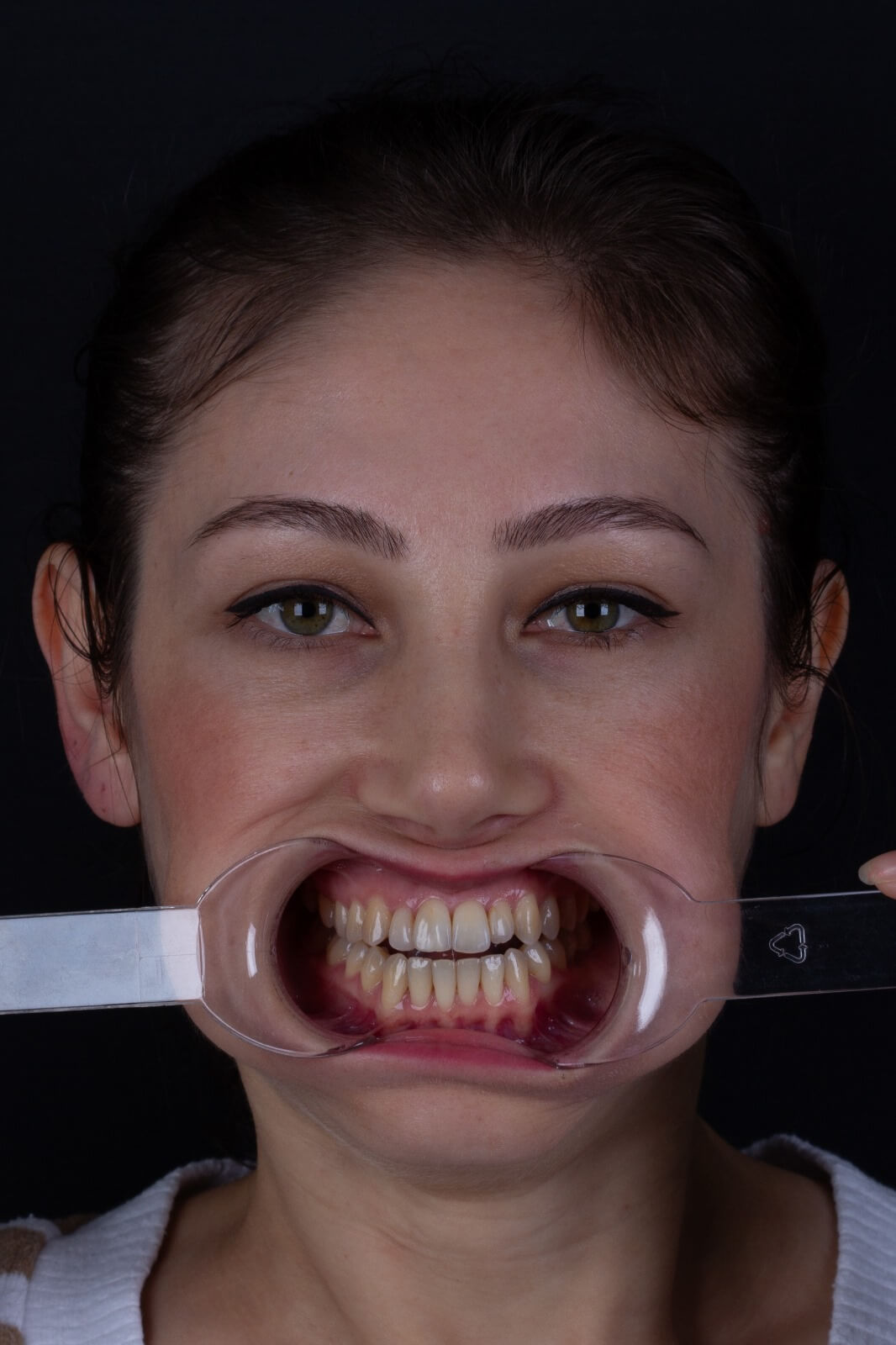
The scanning process should start with a lip-cheek retractor and at the end of the scan, the retractor should be removed to move the scanning head more easily and to scan hard-to-reach areas such as the areas between the brackets and the gums in more detail.
Measurements made on the face are written on the analysis form. You can download the analysis form by following the case submission steps.
We need some reference points to make measurements on the face. These points are
- Soft tissue Glabella (Gn')
- Subnasale (Sn')
- Jaw tip midpoint (Pog')
To make these points visible on the radiograph, radio opaque markers are attached to them. Or, instead of these markers, a very small drop of fluid composite can be placed on the marked spot.
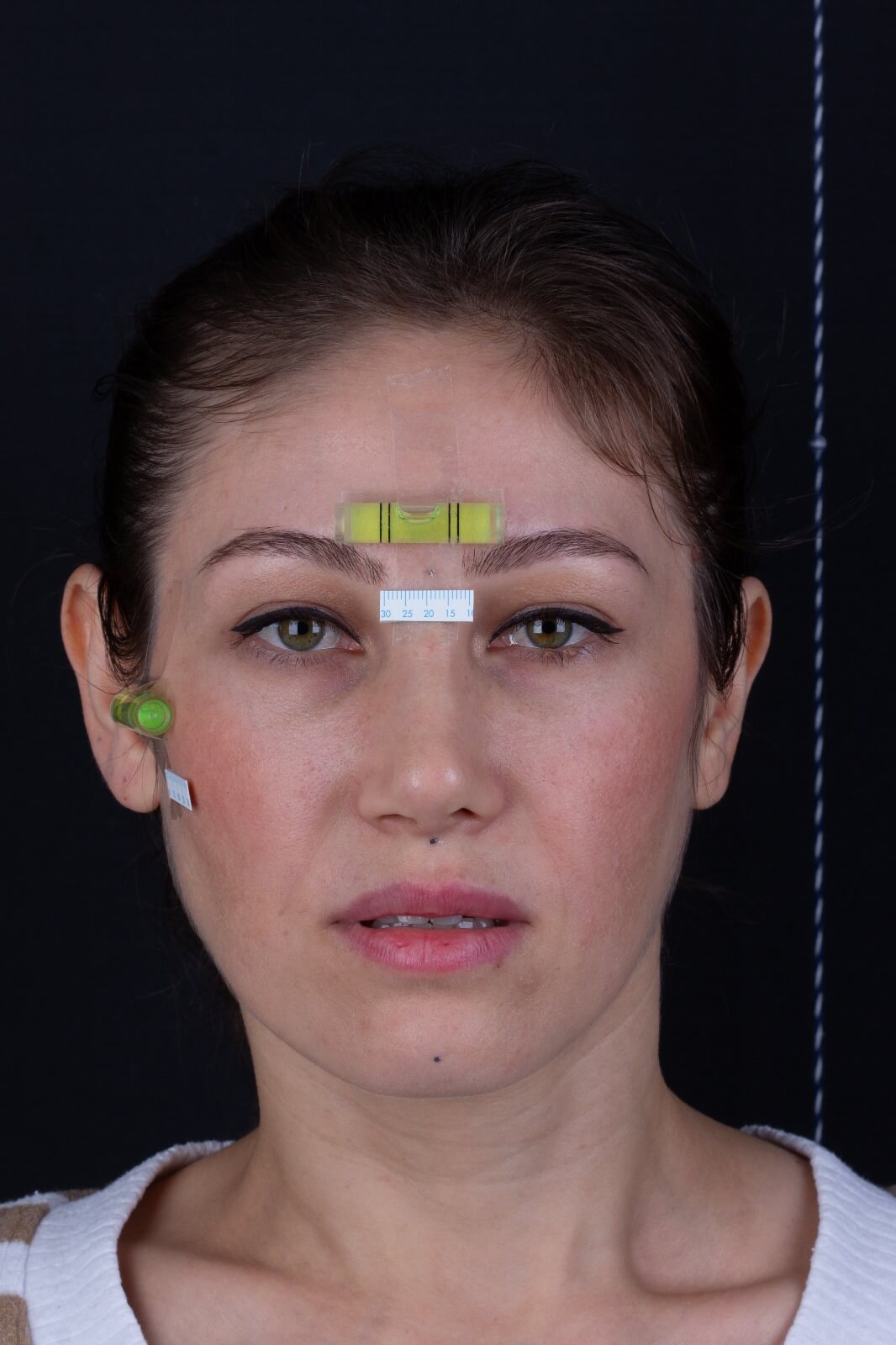
In orthognathic surgery planning, we use the soft tissue cephalometric analysis (STCA) described by Arnett et al. In this analysis, instead of intracranial planes, real vertical and horizontal planes created on the patient's natural head position (NHP) are used as reference. The NHP represents the real-life appearance of the individual and allows us to achieve realistic orthodontic and orthognathic results. Since the DBP can be affected by many reasons, it is often necessary to reposition the patient's head by the physician. This repositioned head position is called natural head orientation (NBO).
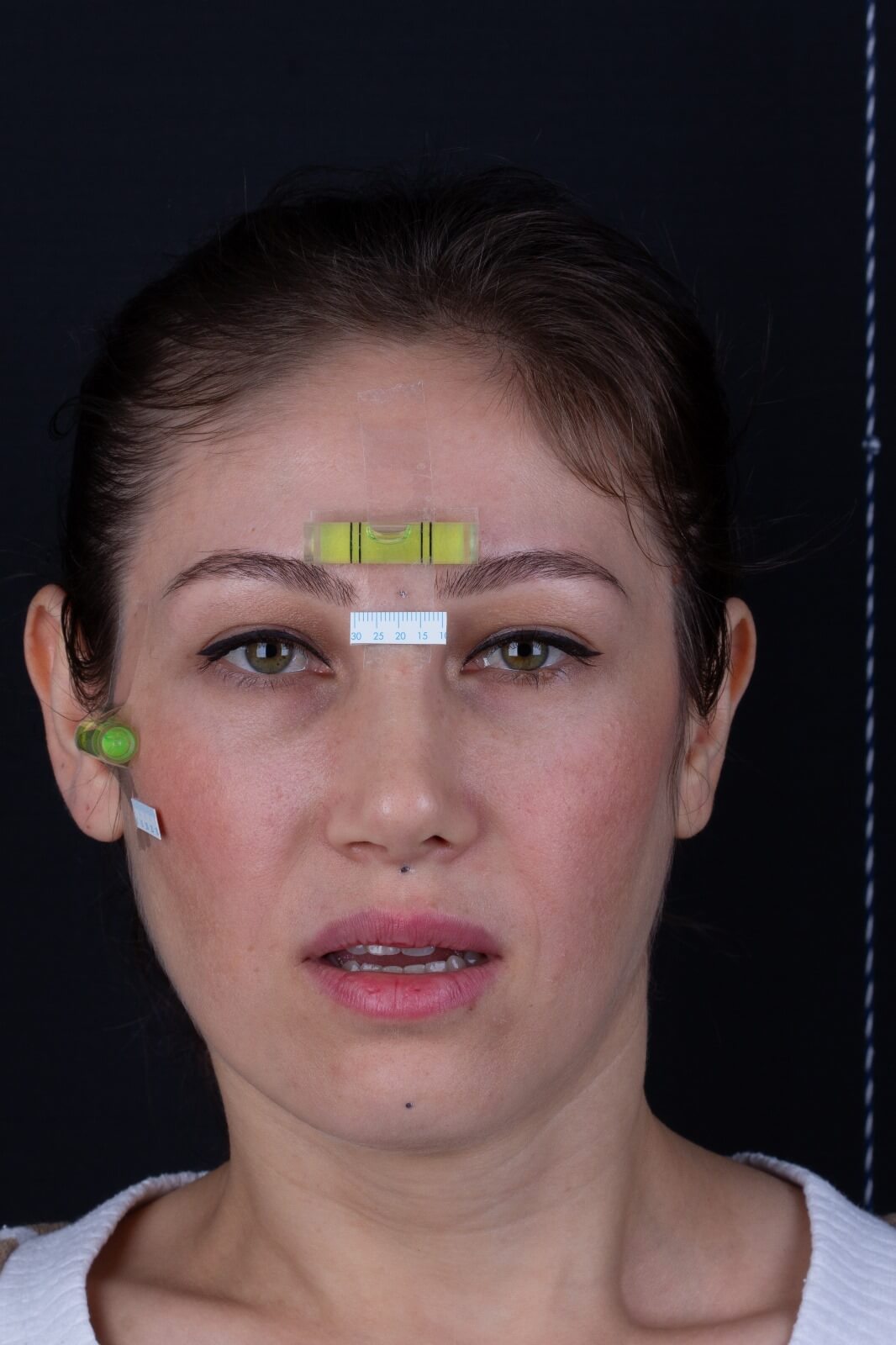
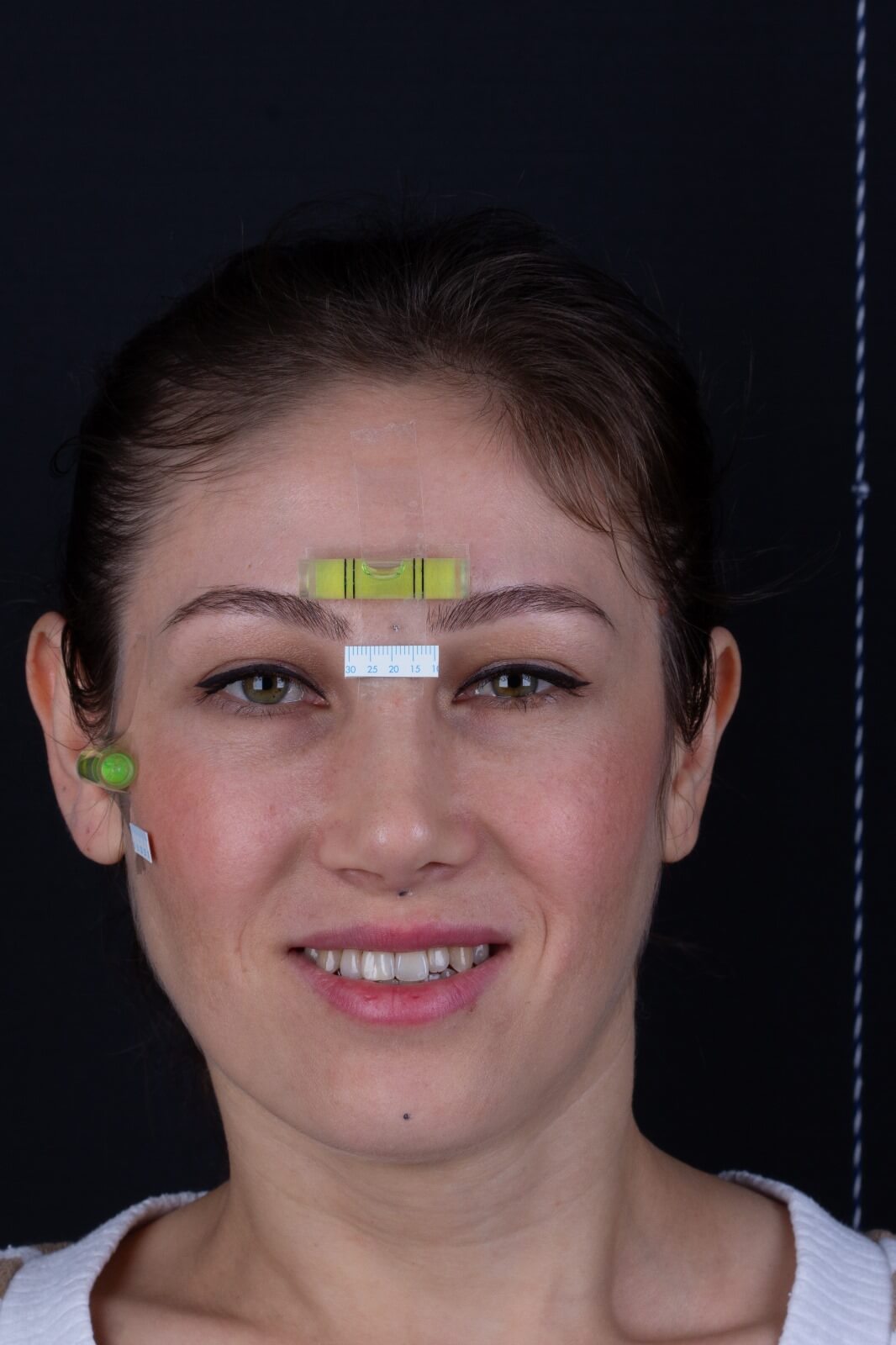
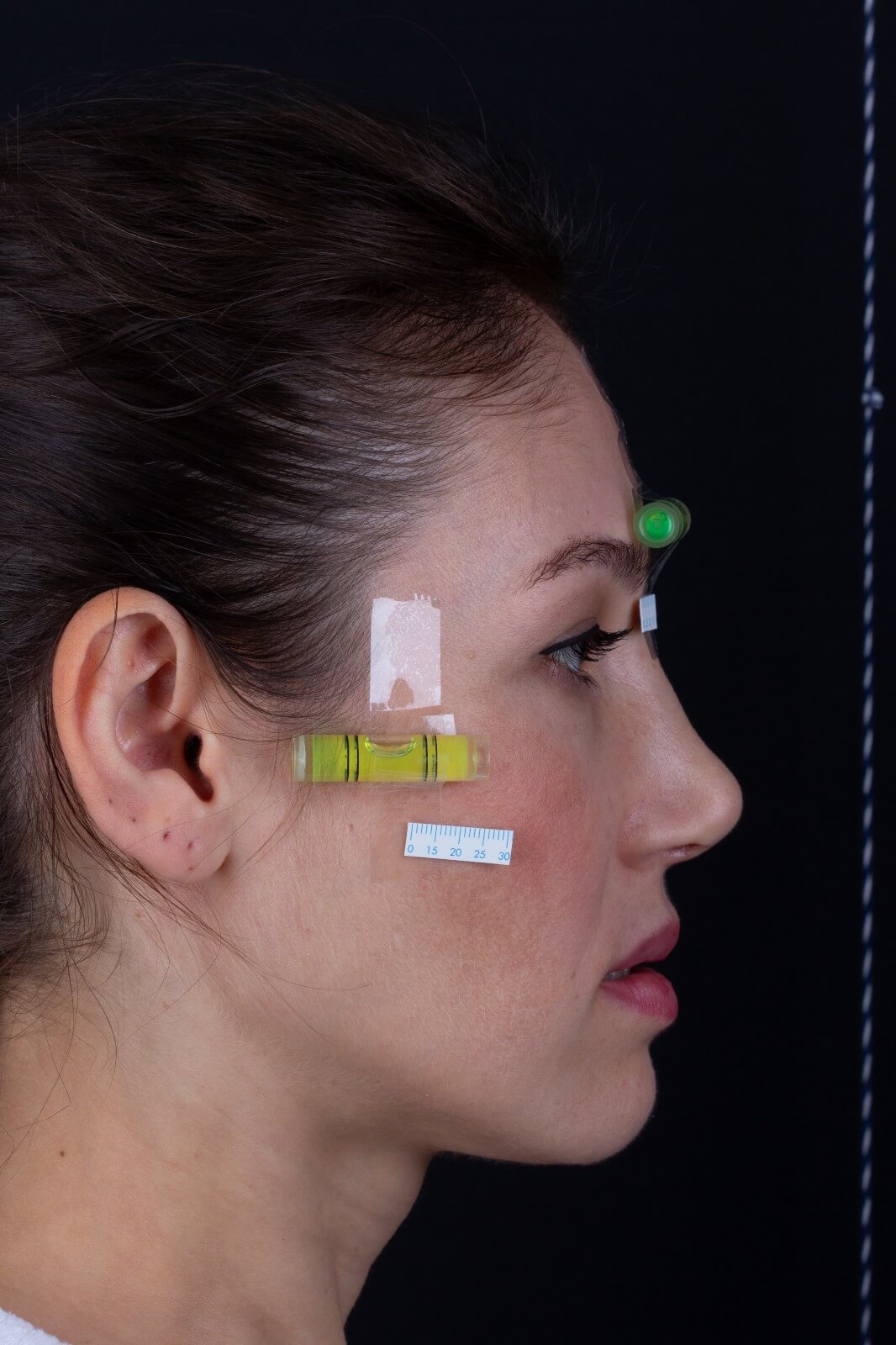
After determining the NHP of the patient, two spirit levels are placed on both the forehead and temporal region with the help of double-sided tape, parallel to the ground plane, while the patient is standing in the NHP so that this position is reproducible. Then, the patient is again asked to walk around comfortably for a while and the head position is repositioned according to the NHP and it is checked whether the spirit levels are parallel to the ground plane. If there is any doubt about the patient's NHP, the spirit levels are removed from the adhesive tape and the procedure is repeated from the beginning.
By making the NHP repeatable using spirit levels, it is possible to take all records securely in the NHP. In this way, the possibility of making mistakes during the transfer of the NHP we have determined in the clinic to the virtual environment is significantly reduced.
(If you wish, we can send a spirit level to your address)
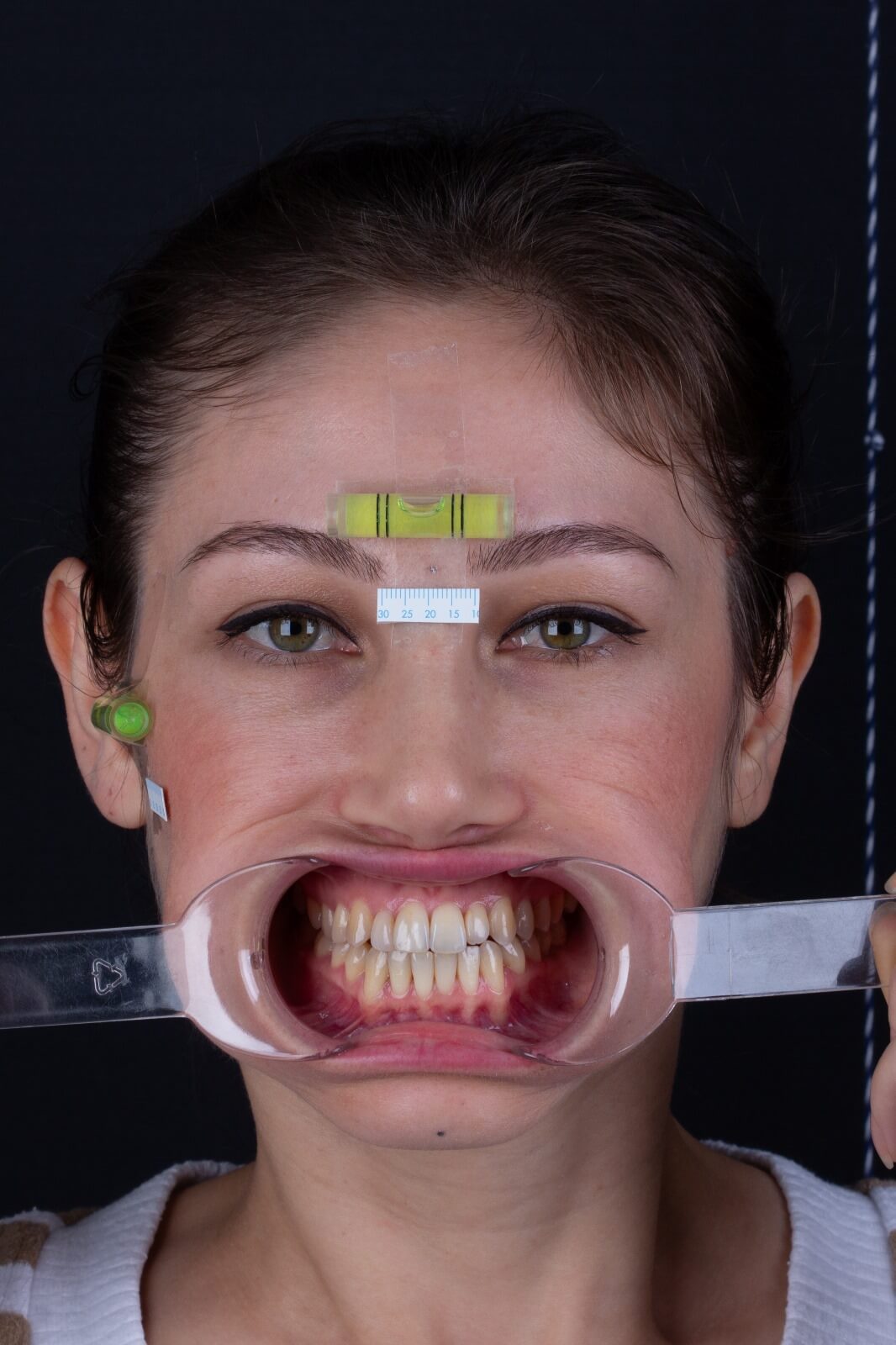
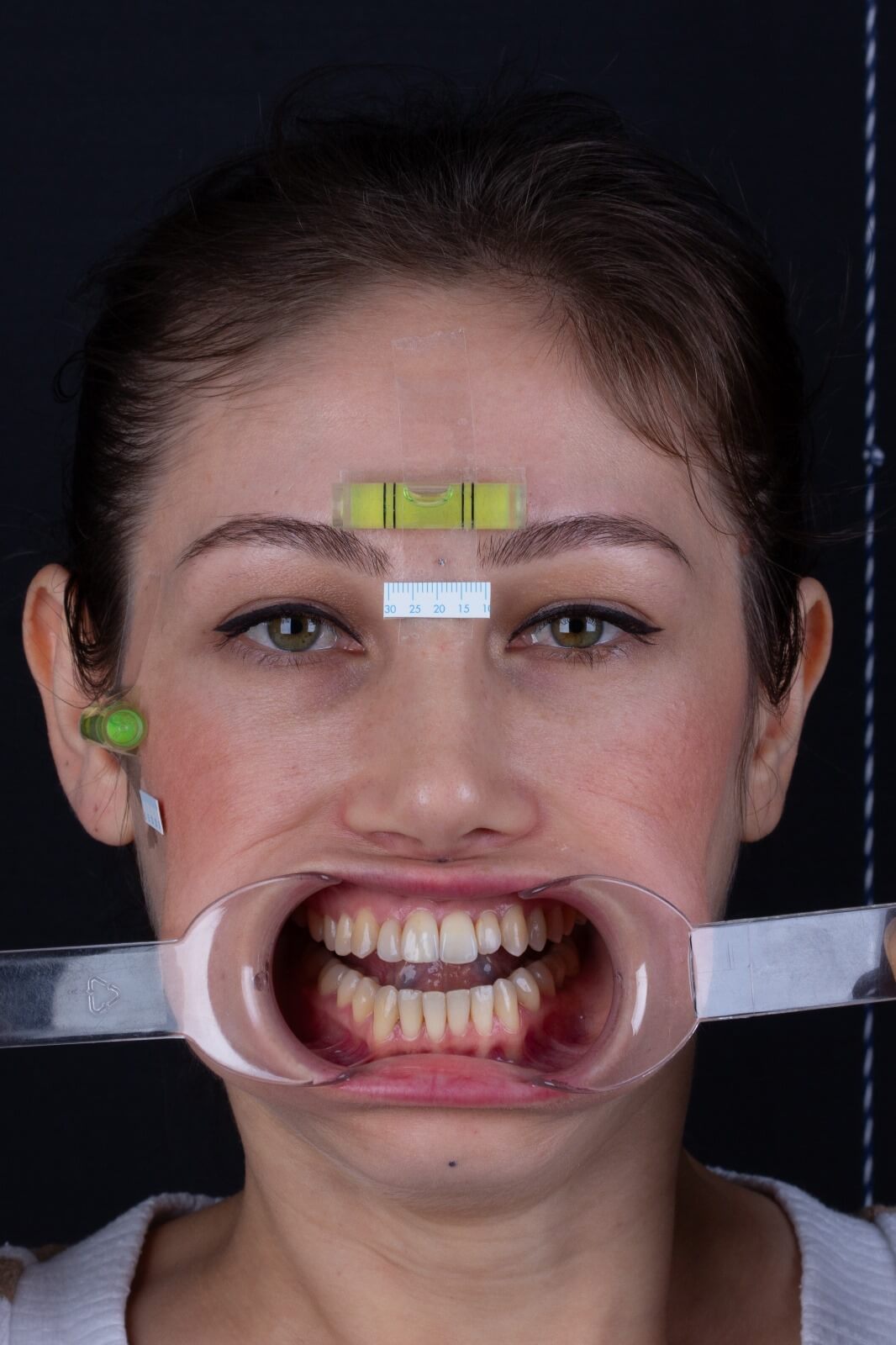
In the clinic, dental floss can be used to determine the midline. The patient's head is held parallel to the ground plane with reference to the spirit level adhered to the patient's forehead, and the floss is held perpendicular to the ground so that it passes over the mark at the 'G' point that we have previously determined, trying to see where the floss passes through the upper incisors. The location is marked on the upper incisors and the accuracy of the mark placed is tested by repeating the process. We recommend that this procedure is done more than once, and if there is a physician working in your clinic other than you, we recommend that he/she also checks this mark.
The vertical distance between the upper canines is tried to be determined by using a ruler or a graduated rod that can measure the cant, while the patient's head is kept parallel to the ground plane with reference to the spirit level adhered to the patient's forehead.
(If you wish, we can send you the stepped bar in STL format to your e-mail)
The closing record will be used when the patient is photographed and radiographed. Thus, during both recordings, the patient's interjaw relationship will be the same as the relationship we determined in the clinic. It is important that the closing wax is not easily deformed when taking the closing record. Therefore, preferably a hard blue wax, similar to kerr material, or a pink wax that has been soaked in ice water and hardened well is used.
The closing wax should not touch the lips and soft tissues.
Before taking photographs, plastic rulers 0.5 mm apart and preferably 20 mm long are glued to the patient's face, just below the spirit levels. In this way, the photographs can be calibrated on the computer.
The closing candle is placed between the teeth.
Both spirit levels on the patient's head should be parallel to the floor during the photographs. While you are taking the photograph, your assistant can guide the patient's head so that the spirit levels are parallel to the floor.
Lips and soft tissues should be free during photography.
The camera lens should be held at eye level.
We recommend the use of a lens hood for clearer photographs. A backdrop should be used and the backdrop should have a reference line perpendicular to the ground plane. We recommend hanging a rope with a weight attached to the end and placing it in the frame. Thanks to the rope swinging from top to bottom, it will be possible to adjust the photo we have taken on the computer so that it is perpendicular to the ground plane.
After the photo shoot, the rulers are removed.
Cone beam computed tomography uses lower radiation doses than conventional computed tomography (CT). Therefore, it is safer to use. It also allows us to obtain all the radiological images we can use during our planning with a single irradiation.
It is recommended that the patient goes to the CBCT scan with water scales on their face. This way, the patient's head can be held in the NHP during the CBCT scan.
The C.B.C.T. must be sent in DICOM format.
Points to be considered when taking C.B.C.T. (recommendations to be expressed to the technician)
- The closing of the teeth should be provided with a closing wax.
- Lips should be free.
- There should be no pressure on soft tissues.
- The chinrest on the machine should not be used.
- The marks on the soft tissue should be visible.
- The glabella point, the point where the lower jaw meets the neck, the tip of the nose and the ears must remain within the FOV (Field of View) area.
- Head position should be adjusted according to the NHP.
- The head should be stabilized.
When you scan the models obtained before surgery by bringing them to the occlusion you want to see during surgery, the patient's final occlusion is obtained. Thus, the final occlusion during three-dimensional virtual surgery planning is determined.
Once we receive the records you have collected, we organize them virtually, analyze them and finalize the surgical planning. We then hold an online meeting where we inform you and the surgeon and finalize the plan.
After agreeing on the surgical plan, we prepare the splints to be used during the surgery and send them to your address.
Explanation and Helpful Sample Photos for Photos





















Frequently
Asked Questions
Contact us;
You can contact us by filling out the form below and we will get back to you as soon as possible.

It refers to the planning of the patient's facial structure using computerized technology before orthognathic surgical interventions.
Virtual face planning involves processing and analyzing data about the patient's facial structure obtained using computed tomography (CT) or Cone Beam Computed Tomography (C.B.C.T.), 3D scanning of teeth and photographs through computer programs. This allows surgeons to examine the patient's facial structure in detail and plan the surgical intervention in advance. Being able to foresee the early bone contacts and anatomical constraints they will encounter during surgery in a virtual environment allows a less invasive approach to be adopted during surgery and helps the patient to have a more problem-free and faster postoperative recovery process. In addition, the images obtained with virtual face planning allow us to better explain the treatment plan to the patient.
3D Printer: Formlabs 3B+
Model printing V3 Model Resin
Splint printing Bioclear Resin
You can always send us your questions to info@sayinsudigital.com or contact us via live support.

